Diagnosis of the syndrome can be made at birth based on physical characteristics, but a true medical diagnosis is confirmed following a diagnostic test called fluorescence in situ hybridization (FISH). The test reveals a recurring micro-deletion, with a size of 1,551,83 Mb, on chromosome band 7q11.23, which contains 24-28 genes.The deleted part of the chromosome band includes the elastin gene, which leads to serious cardiovascular complications. Elastin is a protein responsible for tissue elasticity.0
Other common names for William's Syndrome:
- Williams-Beuren Syndrome
- Beuren Syndrome
- Elfin Facies Syndrome
- Elfin Facies with hypercalcemia
- Hypercalcemia-Supravalvar Aortic Stenosis
- Infantile hypercalcemia
- Supravalvar aortic stenosis syndrome
- WBS
- WMS
- WS
Prevalence
Stated as being anywhere from 1/7,500 to 1/50,000. William’s Syndrome occurs sporadically and spontaneously and is found equally in all ethnicities, races, socioeconomic backgrounds and genders.
Characteristics/Clinical Presentation
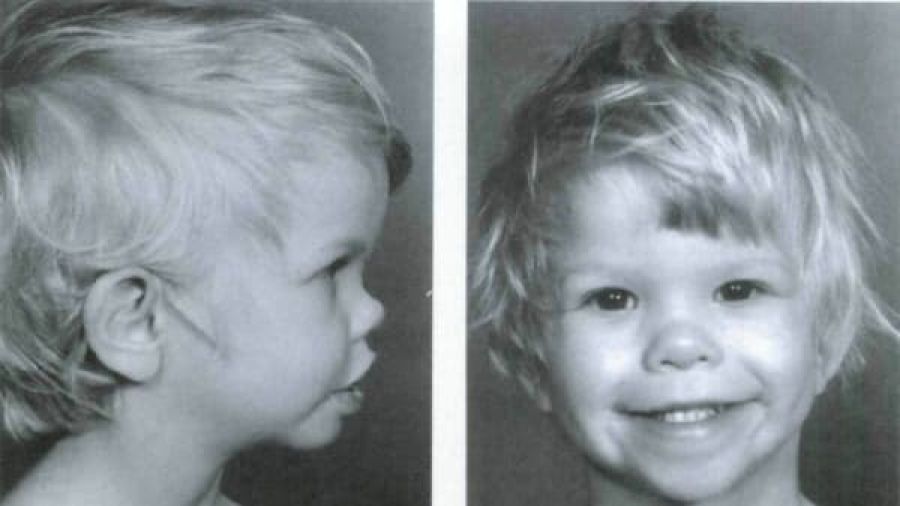
- Craniofacial dysmorphic features
- Full lips, short nasal bridge, large forehead, long philthrum, epicanthal folds, hypertelorism, mandibular hypoplasia
- Mild to moderate mental retardation
- Average IQ = 55-60 but can range from 40-90
- Mild to moderate learning disabilies2
- Associated systemic disorders (especially cardiovascular)
- Mild growth retardation, short stature
- Commonly overweight as adults
- Deficient visuo-spatial abilities
- Global processing deficits
- Overfriendly personalities
- Very sociable
- Empathetic
- High anxiety
- Attention deficit disorder
- Hyperacusis or algiacusis
- White star shape in the iris of the eye
- Increase prevalence of left hand and eye dominance (especially in males)
- Interest and connection with music and sound
Characteristics commonly seen during Infancy:
- Often born post-term
- Small for the family background
- Feeding difficulties - Gastro-esophageal (G-E) reflux, disordered suck and swallow, textural aversion, vomiting
- Failure to thrive
- Prolonged colic (>4 months)
- Chronic constipation
- Idiopathic hypercalcemia
- Strabismus
- Chronic otitis media
- Rectal prolapse
- Inguinal hernia
- Hypotonicity
- Hyperextensible joints
- Delayed motor milestones
Systemic Involvement
Cardiovascular pathologies
- Supravalvular aortic stenosis
- Hypertension
- Ventricular septal defect
- Patent ductus arteriosus
- Stenosis of outlying arteries (renal, cerebral, carotid, coronary, brachiocephalic, subclavian, mesenteric, lung)
- Stenosis of the abdominal aorta
- Arteriovenous shunt
- Interruption of the aortic arch
- Vein aplasia
- Aortic aneurysm
- Pulmonary arterial stenosis
- Left and right ventricular hypertrophy
- Aortic coarctation
- Mitral valve prolapse
- Aortic valvular insufficiency
Endocrine abnormalities
- Hypercalcemia
- Abnormal glucose metabolism
- Thyroid hypoplasia
- Hypothyroidism
Dental anomalies
- Small, abnormally shaped teeth
- Absent teeth
- Malocclusion
Gastrointestinal problems
- Dysmotility
- Reflux
- Constipation
- Diverticular disease
Musculoskeletal anomalies
- Joint laxity
- Joint stiffness as patient ages
- Tight heel cords
- Scoliosis
- Cervical kyphosis
- Exaggerated lumbar lordosis
- Radioulnar synestosis
- Gait - wide BOS, toe-walk, forward posture
Senses
- Sensorineural hearing loss
- Farsightedness
- Hyperopia
- Strabismus
- Otitis media
Genitourinay anomalies
- Urinary frequency
- Bladder diverticuli
Neurological problems
- Abnormal tone
- Hyperreflexia
- Cerebellar dysfunction
- Developmental delays
- Learning disabilities
- Seizures
Medications
There are no medications for William’s Syndrome itself, however, common medications for systemic complications may include: thyroxine for hypothyroidism and thyroid hypoplasia, medication for attention deficit disorder, medication for hypertension, oral corticosteroids and/or intravenous pamidronate for hypercalcemia.
IMPORTANT NOTE: Children with William's Syndrome should not be given a daily pediatric multivitamin because of the dose of vitamin D contained in the vitamin. This can lead to hypercalcemia.
Diagnostic Tests/Lab Tests/Lab Values
The most common test used to diagnose William’s Syndrome is fluorescence in situ hybridization (FISH), but targeted mutation analysis can also be used. Targeted mutation analysis may include any of the following tests: Real-time quantitative PCR, Genomic microarray analysis, and Heterozygosity testing.
Other tests to diagnose systemic complications include: electrocardiogram, echocardiogram, aortography, ultrasonography, Tc-pertechnetate thyroid scintigraphy, thyroid function tests, MRI, polysomnography
There is also prenatal testing available for couples with a family history of Williams syndrome who may want to conceive.
Etiology/Causes
William's Syndrome is a result of a spontaneous microdeletion of a band on chromosome 7. The deletion can be inherited from either the mother or father of a person with William's Syndrome and a person with William's Syndrome has a 50% chance of having a child with the genetic disorder. However, the disorder mostly occurs spontaneously and equally amongst all races, ethnicities, socioeconomic backgrounds and genders. With William's syndrome penetrance is 100%, 100% of people with the gene deletion will have William's syndrome. However, expression of the phenotypic features is variable, thus not every person with William's syndrome will have all of the common characteristics typically seen in those with the disorder.
Associated Co-morbidities
- Supravalvular aortic stenosis
- Hypercalcemia
Medical Management
- Early intervention programs
- Special education programs
- Vocational training to address developmental disabilities
- Speech/language therapy
- Physical therapy
- Occupational therapy
- Sensory integration therapy
- Psychologic evaluation
- Psychiatric evaluation
- Behavioral counseling - often used to manage behavior problems, especially attention deficit disorder and anxiety
- Psychotropic medication - often used to manage behavior problems, especially attention deficit disorder and anxiety
- Surgery may be required for supravalvular aortic stenosis (required in 30% of children with the disorder[9]), mitral valve insufficiency, or renal artery stenosis
- Treatment of hypercalcemia - diet modification, oral corticosteroids, and/or intravenous pamidronate
- Referral to a nephrologist - for management of nephrocalcinosis, persistent hypercalcemia and/or hypercalcuria
- Infants may benefit from feeding therapy
- Corrective lenses - hyperopia
- Patching one eye of surgery - strabismus
- Tympanotomy tubes - otitis media
- Dental cleanings every 3 months
Yearly Check-ups for children with William's syndrome should include the following:
- Medical evaluation
- Vision screening
- Measurement of blood pressure
- Calculation of calcium/creatine ratio in a random spot urine
- Urinalysis
Periodic evaluations for children with William's syndrome should include:
- Serum concentration of calcium
- Thyroid function
- Hearing
- Renal and bladder ultrasound
Periodic evaluations for adults with William's syndrome should include:
- Glucose tolerance
- Cardiac evaluation - mitral valve prolapse, aortic insufficiency, arterial stenosis and other associated cardiac pathologies
- Ophthalmologic evaluation - cataracts
Physical Therapy Management
Dr. Colleen A. Morris suggested adding exercise and joint ROM into the treatment plan for children and adults with William's syndrome in order to help maintain proper blood glucose levels to prevent insulin resistance or the development of diabetes and prevent contractures.
A case study that examined the motor development of children with William's syndrome suggests that due to the deficits found, "early evaluation of motor development, strengthening of motor performance and upper limb dexterity may be vitally important during pre-school and school age."
At Combine Sections Meeting (CSM) 2011, The Children's Hospital of Philadelphia gave a presentation on connective tissue disorders and how to treat them with both land-based and water-based exercise programs. William's syndrome was one of the disorders included in this presentation. The following information about physical therapy treatment for children with William's syndrome was taken from the aforementioned presentation given by Michael Dilenno, PT, DPT, CSCS and Abby Leibrand, PT, DPT.
Typical areas of weakness found:
- Trunk/core
- Shoulder
- Hand
- Hip
- Foot and ankle
Therapeutic Exercises used to treat the above weaknesses include:
- Strengthening
- Stretching
- Neuromuscular Re-education
- Neuromuscular Stabilitization
- Functional Training (self-care and home management)
- Functional Training in job/school/play
- Devices and equipment
The following muscles or muscle groups were targeted during strengthening treatment sessions:
- Abdominal exercise
–Transverse Abdominus
–Obliques
–Lower Abdominals - Back
–Extensors
–Latissimus dorsi - Shoulder girdle and attachments
–Middle Trapezius
–Lower Trapezius
–Rhomboids
–Serratus Anterior - Muscles of or influencing the elbow, hand, hip, knee, ankle and foot
Examples of methods for treating weaknesses include using the following:
- For infants, toddlers, children
–Physioball activities for trunk and core
–Increase resistance with t-band, weight, objects - For older children, adolescents, young adults
–Physioball
–Resistance bands
–Free weights
–Machines
Differential Diagnosis
Dr. Colleen A. Morris stated that William's Syndrome "should be distinguished from other syndromes that include developmental delay, short stature, distinctive facies, and congenital heart disease."
Syndromes that should be distinguished from William's Syndrome include:
- Noonan Syndrome
- Deletion 22q11 (DiGeorge syndrome)
- Smith-Magenis syndrome
- Kabuki syndrome
- Fetal Alcohol Syndrome (FAS)








