Function
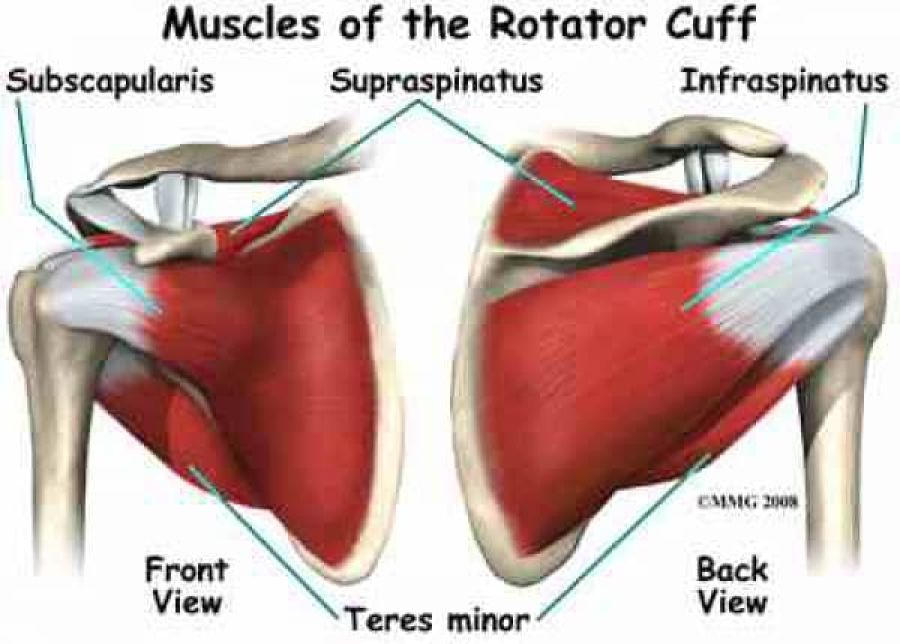
The RC muscles are each used in a variety of upper extremity movements including flexion, abduction, internal rotation and external rotation. They are essential players in almost every type of shoulder movement. Balanced strength and flexibility in each of the four muscles are vital to maintain functioning of the entire shoulder girdle.
As a group, the rotator cuff muscles are responsible for stabilizing the shoulder joint, by providing the "fine tuning" movements of the head of the humerus within the glenoid fossa. They are deeper muscles and are very active in the neuromuscular control of the shoulder complex during upper extremity movements.
They keep the head of the humerus within the small glenoid fossa of the scapula in order to enlarge the range of motion in the GH joint and avoid mechanical obstruction (i.e. a possible biomechanical impingement during elevation).
It is well documented that RC dysfunctions can lead to shoulder pain, impaired functional capacities and a reduced quality of life.
Common Injuries to the Rotator Cuff
RC injuries are common injuries that can occur at any age. In younger subjects, most injuries occur secondary to trauma or arise from overuse due to overhead activities (e.g. volleyball, tennis, pitching). Incidence of injuries increases with age, however some individuals with rotator cuff pathology may be asymptomatic. The RC muscles can fall victim to muscle degeneration, impingement and tearing with advancements in age. Poor biomechanics, such as postural dysfunctions (anterior posture of the GH in the glenoid cavity, for example) can prematurely affect the quality of the RC muscles and tendons due to repetitive strains and tissue encroachment.
Most common injuries to the Rotator Cuff are often referred to as:
- Rotator Cuff Tears (micro or macro tearing of the muscles or tendons);
- Rotator Cuff Tendinitis (acute inflammation of the RC soft tissue);
- Rotator Cuff Tendinopathy (chronic irritation or degeneration of the RC soft tissue);
- Impingement syndrome (biomechanical dysfunction of the shoulder complex with causes abnormal wear and tear on the RC soft tissue).
Common Symptoms
It is important to note that RC tears or injuries are not always associated with pain or patient-reported loss of function. Moreover, it is worth noting that asymptomatic patients may develop symptoms in a relatively short period of time.
The most common signs of rotator cuff injuries are:
- Pain (may or may not be present). Can be localized to anterior / lateral aspect of the shoulder, with referred pain down the upper arm (lateral aspect).
- Painful range of motion
- Painful arch (degrees vary - generally above shoulder height)
- Painful external rotation / internal rotation / ABDuction
- Muscle weakness in the shoulder joint (particularly ABDuction and ER)
- Functional impairments (difficulty lifting, pushing, overhead movements and movements with hand behind the back).
These signs result mainly from a loss of the superior stability of the glenohumeral joint because of dysfunction of the rotator cuff muscles.
Diagnosis of Rotator Cuff Pathologies
Key elements in diagnosing RC pathology are:
- History
- Age / sex / co-morbididies (diabetes / smoking / prior shoulder pain / cervical pain)
- Participation in sports (contact sports / overhead sports)
- Mechanism of injury (acute injury (ie. Fallen on outstretched hand (FOOSH)) / trauma or repetitive strain)
- Physical Examination
- Visual inspection of the shoulder / cervical and thoracic spine
- C-spine scan (rule out referred pain and/or radiculopathy)
- Palpation (pain/deformity/swelling)
- Range of motion / functional movements
- Strength testing (manual muscles testing or with a hand held dynamometer)
Clinical Tests: The diagnosis of an RC tendinopathy can be done in a clinic with the use of Cluster Tests:
The following Cluster Tests were retrieved from Roy et al. (2015):
- Hawkins-Kennedy test
- Neer's test
- Painful arch sign
- Empty can test
- Pain or weakness with external rotation.
- Diagnostic imaging of the shoulder:
- X-rays (less accurate for RC diagnosis; unless a suspected avulsion fracture, calcifications, arthritis or bone deformities)
- MRI (best practice for visibility of soft tissue) or
- Ultrasound (US)
It is important to differentiate shoulder pain coming from places other than the shoulder, such as the neck (referred cervical or thoracic pain) or elbow, and also pains from other structures at the shoulder, through anamnesis and physical examination. Pain is mostly provoked by overhead maneuvers and weakness of the shoulder muscles may occur.
RC muscles can not be seen on X-rays but calcifications, arthritis or bone deformations - that are common causes for rotator cuff pathologies - may be visible. The most common imaging method to evaluate rotator cuff pathologies is MRI. It can detect tears and inflammation and may help to determine size and character in order to establish a proper treatment protocol.
Although, MRI is the gold standard imaging method for rotator cuff pathologies, US can be used as it has a good diagnostic accuracy (Evidence level 2a), more cost effective and readily available.
Possible confounding factors:
- Increase in age;
- MRI tear characteristics;
- Worker's compensation status.
Factors, such as age, chronicity, and severity of muscle tendon unit impairments, have been repeatedly associated with higher retear rates and poorer clinical outcomes.
Possible co-morbidities:
- Diabetes;
- Smoking;
- Prior shoulder infection;
- Cervical disease.
Common Treatments for Rotator Cuff Pathologies
Pain management
- NSAIDs, Moderate strength (benefit exceed the potential harm) for use in the absence of a full thickness tear.
- Activity modification, ice, heat, iontophoresis, TENS, PEMF, phonophoresis. Strength of recommendations: inconclusive.
Conservative treatments
- Physiotherapy / exercise prescription / modalities. Inconclusive strength.
- Conservative treatment is effective for many rotator cuff injuries and comprises injecting corticosteroid (or sodium hyaluronate) into the subacromial space and physical therapy to increase the strength of residual muscles and ameliorate shoulder stiffness.
- Corticosteroid injections. Strength of recommendations: inconclusive.
Surgical repair for acute RC tears
To obtain anatomic healing, the torn rotator cuff tendons must be repaired. Surgical repair has shown moderate to excellent clinical results in most studies. However, surgical treatment for chronic and large rotator cuff tears needs to be improved, especially for those in elderly patients, who continue to demonstrate high failure rates.
For irreparable rotator cuff tears, alternative treatments include:
- Superior capsule reconstruction;
- Reverse total-shoulder arthroplasty;
- Acromioplasty;
- Partial RC repair, debridement or muscle/tendon transfer (when irreparable RC tears);
- Allographs and xenographs.








