It should be remembered that only 5% of people suffering from tennis elbow relate the injury to tennis! Contractile overloads that chronically stress the tendon near the attachment on the humerus are the primary cause of epicondylitis. It occurs often in repetitive upper extremity activities such as computer use, heavy lifting, forceful forearm pronation and supination, and repetitive vibration. Despite the name you will also commonly see this chronic condition in other sports such as squash, badminton, baseball, swimming and field throwing events. People with repetitive one-sides movements in their jobs such as electricians, carpenters, gardeners , desk bound jobs also commonly present with this condition.
Clinically Relevant Anatomy
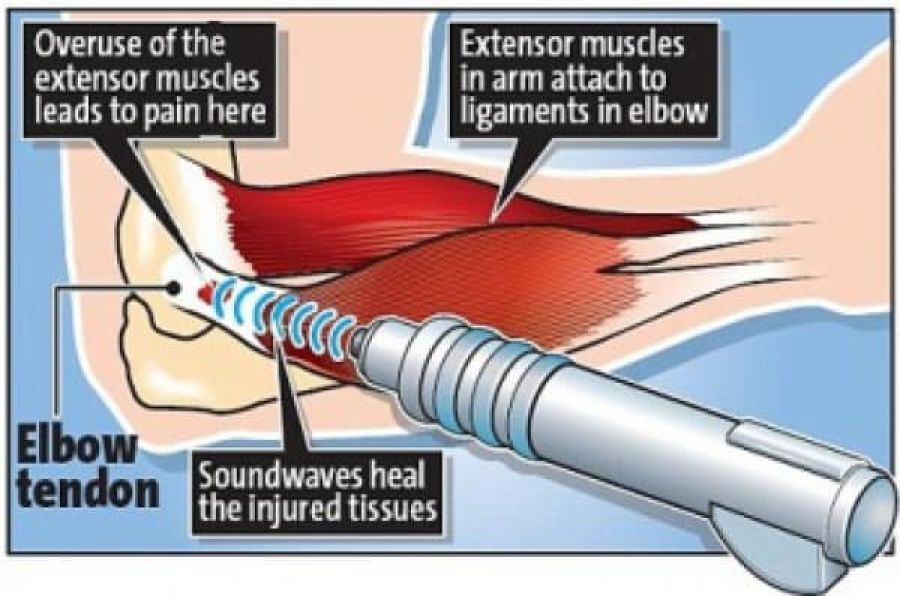
The elbow joint is made up of three bones: the humerus (upper arm bone), the radius and ulna (two bones in the forearm). At the distal end of the humerus there are two epicondyles, one lateral (on the outside) and one medial (on the inside).
The area of maximal tenderness is usually an area just distal to the origin of the extensor muscles of the forearm at the lateral epicondyle. Most commonly, the extensor carpi radialis brevis (ECRB) is involved, but others may include the extensor digitorum, extensor carpi radialis longus (ECRL), and extensor carpi ulnaris.
The radial nerve is also in close proximity to this region, and divides into the superficial radial nerve and the posterior interosseous nerve.
Epidemiology/Aetiology
Lateral epicondylitis is classified as an overuse injury that may result in hyaline degeneration of the origin of the extensor tendon. Overuse of the muscles and tendons of the forearm and elbow together with repetitive contractions or manual tasks can put too much strain on the elbow tendons. These contractions or manual tasks require manipulation of the hand that causes maladaptions in tendon structure that lead to pain over the lateral epicondyle. Mostly, the pain is located anterior and distal from the lateral epicondyle.
Epicondylitis occurs at least five times more often and predominantly occurs on the lateral rather than on the medial aspect of the joint, with a 4:1 to 7:1 ratio. It affects 1-3% of the population, with those 35-50 years old most commonly being affected. If a patient is <35 , it is important to consider differential diagnosis (growth plate disorder, referral from the cervical spine. If a patient is >50, consider OA, referred cervical spine pain. In a study by Nirschl, 1973, of 200 tennis players aged >30, 50% had symptoms of tennis elbow at some stage.
This injury is often work-related, any activity involving wrist extension, pronation or supination during manual labour, housework and hobbies are considered as important causal factors. Lateral epicondylitis is equally common in both sexes. Between the ages of 30-50 years the disease is most prevalent. Obtaining of the condition at the both lateral epicondyle is rare, the dominant arm has the greatest chance of the occurrence of lateral epicondylitis. Twenty percent of cases persist for more than a year.
A systematic review identified 3 risk factors: handling tools heavier than 1 kg, handling loads heavier than 20 kg at least 10 times per day, and repetitive movements for more than 2 hours per day. Other risk factors are overuse, repetitive movements, training errors, misalignments, flexibility problems, ageing, poor circulation, strength deficits or muscle imbalance and psychological factors.
There are several opinions concerning the cause of lateral epicondylitis:
- Inflammation
Although the term epicondylitis implies the presence of an inflammatory condition, inflammation is present only in the earliest stages of the disease process. - Microscopic tearing
• Nirschl and Pettrone attributed the cause to microscopic tearing with formation of reparative tissue (angiofibroblastic hyperplasia) in the origin of the extensor carpi radialis brevis (ECRB) muscle. This micro-tearing and repair response can lead to macroscopic tearing and structural failure of the origin of the ECRB muscle.
• That microscopic or macroscopic tears of the common extensor origin were involved in the disease process, was postulated by Cyriax in 1936.
• The first to describe macroscopic tearing in association with the histological findings were Coonrad and Hooper.
• Histology of tissue samples shows "collagen disorientation, disorganisation, and fibre separation by increased proteoglycan content, increased cellularity, neovascularisation, with local necrosis." Nirschl termed these histological findings bangiofibroblastic hyperplasia. The term has since been modified to bangiofibroblastic tendinosis. He noted that the tissue was characterised by disorganized, immature collagen formation with immature fibroblastic and vascular elements. This grey, friable tissue is found in association with varying degrees of tearing involving the extensor carpi radialis brevis. - Degenerative Process
The histopathological features of 11 patients who had lateral epicondylitis were examined by Regan et al. They determined that the cause of lateral epicondylitis was more indicative of a degenerative process than an inflammatory process. The condition is degenerative with increased fibroblasts, vascular hyperplasia, proteoglycans and glycosaminoglycans, and disorganized and immature collagen. Repetitive eccentric or concentric overloading of the extensor muscle mass is thought to be the cause of this angiofibroblastic tendinosis of the ECRB. Epicondylitis is a degenerative condition in which increased fibrolastic activity and granulation tissue formation occur within the tendon. - Hypovascularity
Because this tendinous region contains areas that are relatively hypovascular, the tendinous unit is unable to respond adequately to repetitive forces transmitted through the muscle, resulting in declining functional tolerance.
Clinical Presentation
The most prominent symptom of epicondylitis lateralis is pain, this pain can be produced by palpation on the extensor muscles origin on the lateral epicondyle. The pain can radiate upwards along the upper arm and downwards along the outside of the forearm and in rare cases even to the third and fourth fingers. Furthermore it is also often seen that the flexibility and strength in the wrist extensor and posterior shoulder muscles are deficient.
According to Warren, there are four stages on the development of this injury with regard to the intensity of the symptoms.
1. Faint pain a couple of hours after the provoking activity.
2. Pain at the end of or immediately after the provoking activity.
3. Pain during the provoking activity, which intensifies after ceasing that activity.
4. Constant pain, which prohibits any activity.
Furthermore it is also often seen that the flexibility and strength in the wrist extensor and posterior shoulder muscles are deficient. At least patients report weakness in their grip strength or difficulty carrying objects in their hand, especially with the elbow extended. This weakness is due to finger extensor and supinator weakness. Some people have a sense of paralysis but this is rare.
Symptoms last, on average, from 2 weeks to 2 years. 89% of the patients recover within 1 year without any treatment except perhaps avoidance of the painful movements .(sport injuries)
Assessment
A thorough assessment and examination are key elements in ensuring that the correct treatment plan is implemented, enhancing the recovery process. The assessment should also include elements to exclude a differential diagnosis.
Subjective Assessment
- Onset of pain 24-72 hours after provocative activity involving wrist extension
- Pain may radiate down forearm as far as the wrist and hand
- Difficulty with lift and grip (Pain+/- weakness)
- Changes in biomechanical factors- new tennis racquet, wet ball, over training, poor technique, shoulder injury
Objective Assessment
- Pain and point tenderness over lateral epicondyle and/or 1-2 cm distal to epicondyle
- Pain and weakness on resisted wrist extension
- Weakness on grip strength testing (Dynamo-meter)
- Pain and/or decreased movement on passive elbow extension, wrist flexion and ulnar deviation and pronation
- Weak elbow extensors and flexors
Differential Diagnosis
- Radial Tunnel Syndrome
• Pain in the posterolateral area of the forearm
• Pain sometimes spreads to the dorsal side of the wrist
• Parasthesia
• Weakness (overuse injuries of the musculoskeletal system) - Posterior Interosseus Syndrome
• Pain
• Weakness involving wrist extension and finger extension
• Motor deficits - Elbow osteoarthritis
• Pain
• Loss of range of motion - Fractures
• Distal Radial Fractures
• Radial Head Fracture
• Olecranon Fracture - Cervical Radiculopathy
• Radiating arm pain corresponding to the dermatomes
• Neck pain
• Parasthesia
• Muscle weakness in myotome
• Reflex impairment/loss
• Headache
• Scapular pain
• Sensory and motor dysfunction in upper extremities and neck - Cervical Disc Disease
- Cervical Myofascial Pain
- Cervical Spondylosis
- Fibromyalgia
- Medial Epicondylitis
Diagnostic Procedures
The diagnose starts with asking about the activity level , occupation risk factors, recreational sports participation, medication and other medical problems. During the physical exam, the medicine will feel the structure of the elbow and other joints. Also the nerves, muscles, bones and skin are examined. It’s important to know which activities cause symptoms and where on your arm the symptoms occur.
Investigations
Investigations are usually not performed in the straightforward case of lateral elbow pain. However, in longstanding cases, plain X-ray (AP and lateral views) of the elbow may show osteochondritis dissecans, degenerative joint changes or evidence of heterotopic calcification.
Ultrasound examination may prove to be a useful diagnostic tool in the investigation of patients with lateral elbow pain. Ultrasound may demonstrate the degree of tendon damage as well as the presence of a bursa.
- X-rays: These may be taken to rule out arthritis of the elbow. 16% calcification along lateral epicondyle
- Magnetic Resonance Imaging (MRI): if the symptoms are related to a neck problem, an MRI scan may be ordered. This will show if there is a possible herniated disk or arthritis in your neck. Both of these conditions often produce arm pain. MRI- 100% thickening
- Electromyography (EMG): An EMG is used to rule out nerve compression. Many nerves travel around the elbow, and the symptoms of nerve compression are similar to those of tennis elbow.
Outcome Measures
- Pain reported outcome measures;
- Numeric Pain Rating Scale (NPRS)
- Visual Analogue Scale (VAS)
- Self-reported Questionnaires;
- The Upper Limb Functional Index (ULFI):
- Patient Rated Tennis Elbow Evaluation (PRTEE):
- QuickDASH (Disabilities of the Arm Shoulder and Hand):
- Patient Specific Functional Scale (PSFS) - although the PSFS has not yet been validated for lateral epicondylalgia, it has been shown to be valid, reliable and responsive to change in other conditions such as knee dysfunction, cervical radiculopathy, acute low back pain, mechanical low back pain, and neck dysfunction (Pain ICC = 0.89-0.99, Function ICC = 0.83-0.99, Total ICC = 0.89-0.99)
Physiotherapy Management
There are different types of therapies to treat lateral epicondylitis, all with the same aim: reduce pain and improve function. General physiotherapy management includes:
- Education/Advice- on pain control and/or modification of activities
- Manual therapy- Mulligan - Mobilisation with movement
- Exercises- Strengthening and Stretching
- Modalities- Ultrasound, Transcutaneous electrical nerve stimulation (TENS)
- Braces/Splints/Straps- No clear evidence
- Medications- NSAIDs offer a short term benefit (3-4 weeks pain relief)
- Corticosteroids injection- Short term effect (<6 weeks)
- Sport/Occupation Specific Rehabilitation








